The fictional MD meets Bill Palmer, the fictional VP of IT Operations
I have an idea for a crossover project where characters from one fictional world meet those in another. Hollywood has done this for years. Some have been more successful than others. For example, there’s the classic straight-to-drive-in-theater Jesse James meets Frankenstein’s Daughter.
On the other end of the box office spectrum is The Avengers where a squad of superheroes saves the earth from catastrophe by working together. I imagine a mashup of the characters in the book, The Phoenix Project and characters from the TV show House MD.
Meet Dr. House
Dr. House is an unconventional, misanthropic medical internist who leads a team of residents and clinicians at the fictional Princeton–Plainsboro Teaching Hospital. House’s snarky personality and dry wit often clashes with his peers. Like Perry Mason who tied up every case at the end of half an hour, House’s insights are apparently based on a secret cache of knowledge that he and only he has access to.
One of the idiosyncrasies that makes Dr. House so watchable is his genius mix of medical aphorisms, clinical acumen, and outlook on life. He has a lot to say about stupidity.
- “Idiots are fun; no wonder every village wants one.”
- “Everybody does stupid things; it shouldn’t cost them everything they want in life.”
- “People can be as overwhelmingly stupid as they want.”
House embraces unconventional methods and prioritizes the end goal over popularity. He uses conflict to foster creativity and teaches through challenge. He does maintain high standards for patient care and insists on excellence.
It is exactly these qualities in Dr. House that make it so interesting when he is confronted with the challenges of IT and is the face of medicine for Bill Palmer.
Meet Bill Palmer
In The Phoenix Project: A Novel About IT, DevOps, and Helping Your Business Win, Bill Palmer takes on challenges many businesses face in real life. The story follows Bill Palmer as he is tapped to lead the IT Team at Parts Unlimited after his bosses have been fired for failing to deliver IT value. We learn in this story as Palmer learns on the job and has his many aha moments. If Dr. House and Bill were to meet, Dr. House would be the foil to challenge Bill. Dr. House might serve as a similar literary figure to the enigmatic Eric character in The Phoenix Project. Eric is like a Yoda who helps Bill find the power and answers within himself.
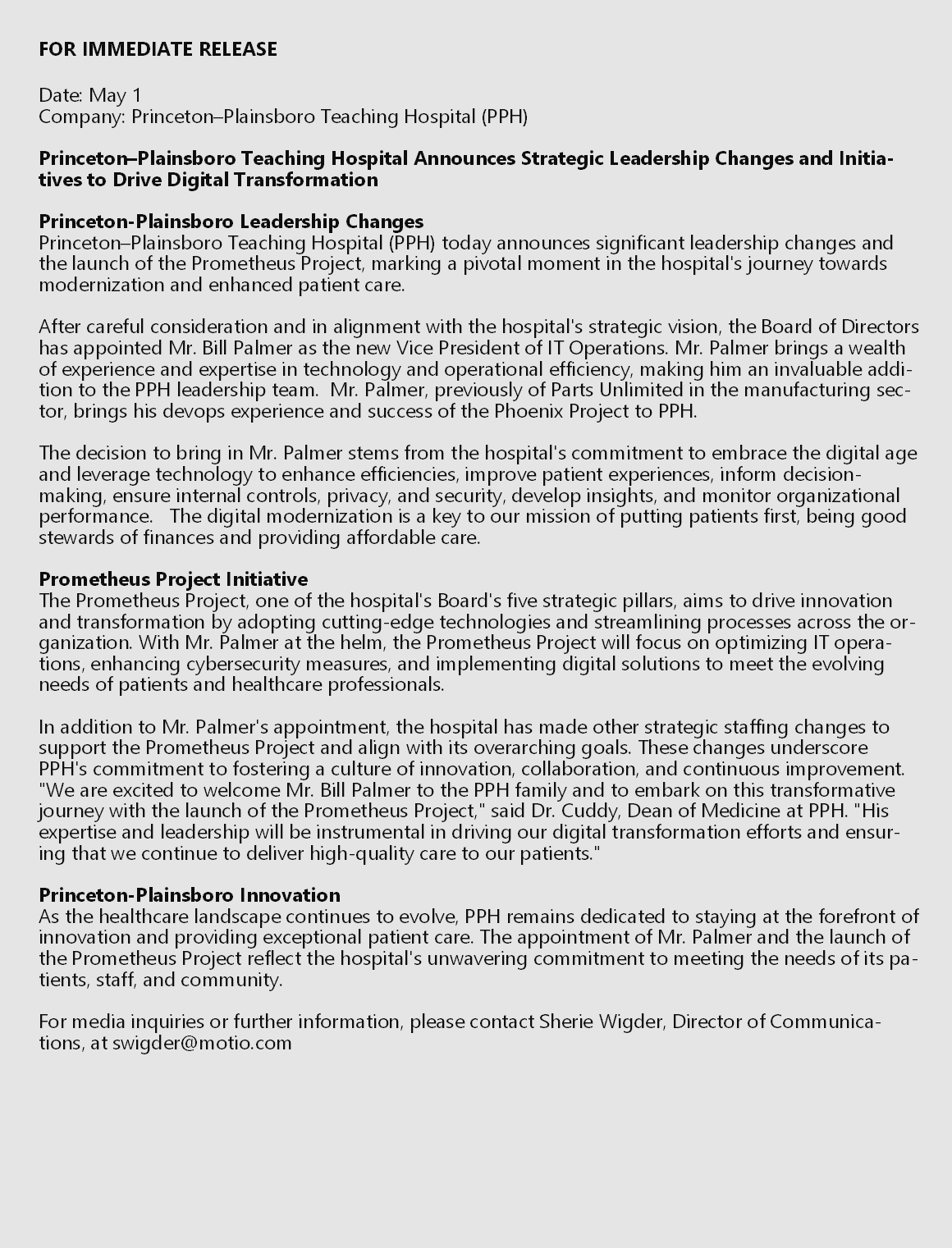
In our fan fiction, Bill Palmer, the VP of IT Operations at Parts Unlimited, is poached by Princeton-Plainsboro Teaching Hospital to turn around similar organizational challenges and technical issues. Princeton-Plainsboro Hospital has an initiative called Project Prometheus that has been having problems that are eerily similar to those encountered in The Phoenix Project.
The Prometheus Project
On his first day at PPH and Project Prometheus, Bill is welcomed by Dr. Cuddy, the Dean of Medicine and hospital administrator. She describes Project Prometheus as critical to modernizing the hospital’s IT systems. Project Prometheus is so important; it is one of the hospital Board’s five strategic pillars, Evolve with the Digital Age: Adopt technologies that enhance efficiencies, improve patient experiences, inform decision-making, ensure internal controls, privacy, and security, develop insight, and monitor organizational performance.
Dr. Cuddy explains that one of the key challenges has been getting buy-in from the professional staff about the changes and the priorities. She strongly recommends that Bill orient himself to the challenges of the project by talking with the physicians who are both consumers of the technology and key stakeholders. Unsurprisingly, first on his list is Dr. Gregory House.
Before he meets Dr. House, Dr. Cuddy introduces Bill to his new team. It’s lean. They fill him in on the Electronic Medical Records upgrade over the weekend. Not everything went to plan.
Bill enters the conference room.
Dr. House: [looks up from his crossword puzzle.] Oh great, another eager beaver wandering into my domain. What do you want?
Bill Palmer: Dr. House, I’m Bill Palmer, the new VP of IT Operations here. I’ve been brought in to work on the Prometheus Project. I hear you’re one of the key physicians I should talk to about the challenges we’re facing.
Dr. House: rolls his eyes Prometheus Project, huh? Sounds fancy. And you want me to spill my precious pearls of wisdom on how to make it all rainbows and unicorns?
Bill Palmer: Well, not exactly rainbows and unicorns, but yes, I’d appreciate your insights. We’re trying to improve efficiency, patient experiences, and all that jazz, and it seems there’s resistance to the changes. Dr. Cuddy said you might have some perspective on that.
Dr. House: [leans back in his chair] So you’re the IT guy who thinks he can fix our problems with his magical tech solutions?
Bill Palmer: I wouldn’t call it magical, but yes, I believe technology can play a role in improving things.
Dr. House: smirks Right, because nothing says “cure” like lines of code. Let me guess, you’re going to tell me DevOps is the answer to all our prayers?
Bill Palmer: Actually, I wanted to clear up some misconceptions about DevOps. Like, for instance, some folks think it replaces everything else, is just an IT thing, or is just for startups. But it’s really about streamlining processes, collaboration, and using technology effectively.
Dr. House: [raises an eyebrow] So, what? You’re going to make our hospital run like a finely-tuned machine with all your tech mumbo-jumbo?
Bill Palmer: Well, not exactly a machine, but yes, the idea is to make things more efficient so that patient care can improve.
Dr. House: Ah, yes, because nothing’s more efficient than a computer telling me how to diagnose a complex medical case. I can just see it now: “Patient has a 404 Error in the left frontal lobe. Please reboot.”
Bill Palmer: [chuckles] I understand your skepticism, Dr. House. But DevOps isn’t about replacing human expertise; it’s about giving you tools to work better, faster, and with fewer obstacles.
Dr. House: [narrows his eyes] Tools, huh? Just like my cane is a tool to annoy Cuddy’s assistants?
Bill Palmer: [laughs] Well, you’ve got quite the analogy there, but yes, tools that can help the hospital function more smoothly and help you focus on what you do best.
Dr. House: [pauses] Look, IT guy, I’ll give you this much – if you can actually make our digital mess less messy and not interfere with my medical Sherlock Holmes routine, then maybe I’ll consider that DevOps stuff of yours as more than just tech voodoo.
Bill Palmer: Fair enough, Dr. House. I appreciate your candor. And rest assured, I’m here to make things better, not to mess with your diagnostic brilliance.
Dr. House: [smirks] Well, we’ll see about that, won’t we? Just remember, I solve medical mysteries; you’re the one who’s supposed to untangle this IT labyrinth.
Bill Palmer: Deal. And hey, if you ever want to see how DevOps can actually work wonders, you know where to find me.
Dr. House: Oh, joy. Another miracle worker in the house. Can’t wait.
====================
The next day, dark o’thirty
====================
Dr. House: [storms into Bill Palmer’s office] Well, well, well. Look who we have here – the tech wizard himself.
Bill Palmer: [looks up from his computer] Ah, Dr. House. To what do I owe the pleasure of this unexpected visit?
Dr. House: [sarcastically] Oh, you know, I just wanted to check on the progress of your glorious Prometheus Project. Heard we’ve got a little glitch in the Matrix.
Bill Palmer: [sighs] Yes, we’ve encountered a problem with the EMR software. There was a virus, and we had to take it offline to patch and clean it up.
Dr. House: [raises an eyebrow] A virus? You mean like the common cold? Maybe we should start vaccinating our computers too.
Bill Palmer: [rolls his eyes] Not that kind of virus, Dr. House. A malicious software that can compromise the security of our patient data.
Dr. House: [smirks and pretends he didn’t know] Ah, the wonders of modern technology. And here I thought Prometheus was going to save us from such nightmares.
Bill Palmer: Look, Dr. House, technology isn’t foolproof. Just like medicine, it’s constantly evolving, and sometimes unexpected things happen.
Dr. House: [leans in] Funny how you IT guys are always quick to compare your world to ours, yet when things go south, you play the “unpredictable” card.
Bill Palmer: [calmly] I’m not trying to make excuses. We’re working diligently to fix the issue and ensure it doesn’t happen again. Just like you do when you’re dealing with a complex medical case.
Dr. House: [crosses his arms] You see, the thing is, when I diagnose a patient, I don’t promise them a magic cure-all solution. But you tech folks, you sell us on this grand vision of a perfectly interconnected hospital world, and then bam – viruses, glitches, chaos.
Bill Palmer: Fair point, Dr. House. I won’t deny that our pitch may have been a bit optimistic. But that doesn’t mean we’re giving up on making things better.
Dr. House: [smirks] So what’s the remedy this time? A software band-aid? Or maybe you’ll send in an army of digital antibodies to fight off those nasty viruses?
Bill Palmer: [smiles] More like a thorough examination, identification of vulnerabilities, patching, and strengthening our defenses.
Dr. House: [pauses] You know, for someone who’s all about DevOps and efficiency, you sound a lot like a doctor. Maybe you should consider a career change.
Bill Palmer: [chuckles] Thanks for the suggestion, Dr. House, but I’ll stick to my tech realm. And I promise you, we’re doing everything we can to get things back on track and keep them that way.
Dr. House: [starts to walk away] Just remember, Palmer, when it comes to technology, even the smartest minds can’t outwit the inevitable chaos. Good luck.
Bill Palmer: [watches him leave] Thanks, Dr. House. And don’t worry, chaos is our middle name. We’ll tame it eventually.
Dr. House: [smirks over his shoulder] I’ll believe it when I see it, IT guy.
======================
======================
Bill Palmer: [approaches Dr. House, who’s engrossed in his whiteboard of medical diagrams and text with circles and arrows] Dr. House, we need to talk.
Dr. House: [doesn’t look up] Ah, the harbinger of more tech troubles? What’s it this time, Palmer?
Bill Palmer: [pauses] Brace yourself, because it’s worse than you thought. The EMR system is going to be down for the entire weekend.
Dr. House: [finally looks at him] You’re kidding, right? The whole weekend?
Bill Palmer: [sighs] I wish I were, but no. We need time to restore the system from backup, thoroughly test it, and ensure it’s stable before bringing it back online.
Dr. House: [sarcastically] Wonderful. So, I assume we’re throwing a weekend-long EMR-themed party?
Bill Palmer: [deadpan] I don’t think it’ll be that much fun. But seriously, Dr. House, we understand the impact this will have on patient care and hospital operations. Unfortunately, it’s the only way to ensure we’re not compromising patient data and system integrity.
Dr. House: [grumbles] Just when I thought dealing with patients was challenging enough. Now I get to channel my inner scribe with pen and paper.
Bill Palmer: [nods, keeping his deja vu moment to himself] I know it’s a huge inconvenience, especially for doctors like you who rely heavily on the EMR system. But the billing system is also tied to the EMR, so if we want to make sure we get paid and keep the financial side running smoothly, reverting to paper charts, orders, and invoicing is the way to go.
Dr. House: [rolls his eyes] Fantastic. I can’t wait to decipher my own handwriting in a week when I need to follow up on a case.
Bill Palmer: [smirks] Well, it might be a good exercise in improving your penmanship. But in all seriousness, we’re working round the clock to get the EMR system back up as soon as possible. And we’ll make sure all the data is secure and accurate before we flip the switch.
Dr. House: [sighs] You better be right about this, Palmer. I don’t have time to play “Guess the Diagnosis” with my own prescriptions.
Bill Palmer: [confidently] We’ll make it happen, Dr. House. Just bear with us for the weekend, and we’ll have everything back to normal soon.
Dr. House: [waves a hand dismissively] Fine, fine. Just don’t mess up. And if my handwriting causes a patient to receive the wrong meds, I’m blaming you.
Bill Palmer: [smiles] Fair enough, Dr. House. I’ll take that responsibility. And hey, maybe you’ll discover a hidden talent for calligraphy in the process.
Dr. House: [mutters] As long as I don’t discover any hidden talent for patience while I’m at it.
Bill Palmer: [chuckles] Understood, Dr. House. Hang in there. We’re on it.
Dr. House: [walks away] Let’s hope your IT magic isn’t as elusive as the diagnoses I deal with.
=========================
As the weekend progressed, the hospital found itself navigating the choppy waters of technological regression. Physicians, accustomed to the instant access and efficiency of the Electronic Medical Records (EMR) system, were forced to rely on the antiquated methods of pen and paper. The atmosphere was tense, with the staff feeling the weight of the digital blackout.
Bill Palmer, despite the mounting pressure, remained a beacon of calm in the storm. His confidence in his team’s ability to resolve the crisis was unshaken. Behind the scenes, his team worked tirelessly, their efforts a blend of technical prowess and sheer determination to restore the EMR system. Their dedication was a testament to the principles of DevOps: collaboration, communication, and continuous improvement.
Meanwhile, Dr. House, ever the skeptic, watched the unfolding drama with a mix of irritation and begrudging respect for Palmer’s optimism. In a rare moment of reflection, House considered the parallels between their work. Both faced complex systems—be it human or digital—where the smallest variable could lead to failure. And both required a blend of knowledge, intuition, and the humility to admit when they were wrong.
On Monday morning, as the hospital braced for another day of manual operations, Bill Palmer entered the IT department with a sense of cautious optimism. Overnight, his team had managed to isolate the last of the vulnerabilities and fully restore the EMR system. But more than just fixing a technical glitch, they had strengthened the hospital’s digital defenses, ensuring that this type of failure would be far less likely in the future.
As the system came back online, a collective sigh of relief swept through the hospital. Physicians and nurses, once again armed with their digital tools, felt a renewed sense of efficiency and safety in their patient care.
Dr. House, upon hearing the news, sought out Palmer. Finding him in the bustling IT department, House offered a nod of acknowledgment—a rare gesture of respect from the diagnostician.
“Looks like your IT voodoo worked after all,” House remarked, his tone carrying a hint of amusement.
Palmer smiled, recognizing the compliment hidden within House’s typical sarcasm. “Just doing our job, Dr. House. But I couldn’t have done it without understanding the importance of what you do here. It’s not just about the technology; it’s about supporting the people who use it.”
House paused, considering Palmer’s words. “Maybe there’s hope for you yet, Palmer. Just remember, in medicine and in IT, the human element is always the most complicated part.”
As Palmer watched House walk away, he couldn’t help but feel a sense of accomplishment. Not just for fixing the system, but for bridging the gap between two worlds that, at their core, were not so different. They were both about solving problems, about making things work better. And perhaps most importantly, they were about recognizing the value of every individual’s contribution to the greater goal.
In the end, the Phoenix Project at Princeton-Plainsboro Teaching Hospital was more than just a technological upgrade. It was a lesson in collaboration, resilience, and the endless pursuit of improvement. And for Bill Palmer and Dr. Gregory House, it was a reminder that medicine and technology have more in common than they do differences.