
Disclaimer
Don’t skip this paragraph. I hesitate to wade into these contentious, often political waters, but a thought came to me while I was walking my dog, Demic. I earned an M.D. and have been in some form of healthcare or consulting since. Over the past 20+ years, I have learned critical thinking. For the IBM team I discuss in the article, I acted as the Data Scientist. I say that I speak the languages of medicine and of data. I am not an epidemiologist or public health expert. This is not intended to be a defense of or critique of any particular individual or policy. What I present here are merely observations. It is my hope to stir your thoughts, as well.
Fighting Zika With Data
First, my experience. In 2017, I was selected by IBM from over 2000 applicants, to participate in a pro bono public health project. A team of five of us were sent to the country of Panama for a month to work with the public health department there. Our mission was to create a digital tool that would facilitate more rapid and effective decision-making related to several mosquito-borne infectious diseases; the main one being Zika.
The solution was an information-sharing pipeline between field investigators and policy makers to control Zika and other infectious diseases. In other words, we developed a mobile application to replace their age-old manual process of sending vector inspectors into the field. Timely, accurate data reduced the outbreak size and duration by being able to better strategically target the areas – think city block – that need remediation.
Since that time, the Zika pandemic has run its course.
Human action didn’t end the Zika pandemic. The public health community worked to contain it, through diagnostics, education and travel advisories. But ultimately, the virus ran its course, infected a large portion of the population, and herd immunity developed, thus halting the spread. Today, Zika is considered endemic in some parts of the world with period breakouts.
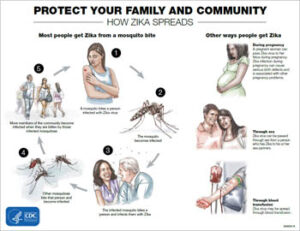 In some of the earliest and deadliest pandemics just about everybody who got sick died. WIth Zika, “Once a large proportion of the population is infected, they’re immune and they actually protect other people from getting infected [there is no vaccine to protect against Zika].” That’s what happened with Zika. The outbreak is over in the Americas and the incidence of Zika now in 2021 is very low. That’s the great news! Zika peaked in 2016 just as the Panama officials asked IBM to send help to combat the mosquitoes. Zika Transmission | Zika Virus | CDC
In some of the earliest and deadliest pandemics just about everybody who got sick died. WIth Zika, “Once a large proportion of the population is infected, they’re immune and they actually protect other people from getting infected [there is no vaccine to protect against Zika].” That’s what happened with Zika. The outbreak is over in the Americas and the incidence of Zika now in 2021 is very low. That’s the great news! Zika peaked in 2016 just as the Panama officials asked IBM to send help to combat the mosquitoes. Zika Transmission | Zika Virus | CDC
Correlation is not causation, but after our visit to Panama, the Zika pandemic continued to wane. There are occasional outbreaks, but it hasn’t since reached the same level of concern. Some expect the pendulum to swing back as natural immunity wanes and unexposed individuals migrate into Zika high risk zones.
Zika and COVID-19 Pandemic Parallels
How does this relate to COVID-19? Both the pathogen that is responsible for both COVID-19 and Zika are viruses. They do have different primary forms of transmission. Zika is mainly transmitted from mosquitoes to humans. There are opportunities for human-to-human transmission, but the main form of transmission is directly from the mosquito.
For the coronavirus, it has been shown that some animals, like bats and deer, do carry the virus, but the main form of transmission is human-to-human.
With the mosquito borne illnesses (Zika, Chikungunya, Dengue fever), one objective of the Panama public health ministry was to minimize exposure to the virus by reducing exposure to the vector. In the US, in addition to the rapidly developed vaccine, the primary public health measures for addressing COVID include reducing exposure and limiting spread to others. Mitigation measures for those who are at high risk have included masking, physical distancing, isolating and closing the bars early.
The containment of both diseases depends on … ok, maybe this is where it gets controversial. In addition to education and sharing data, the public health goals of prevention of the severest outcomes can be focused on 1. eradication of the virus, 2. eradication of the vector, 3. vaccination/protection of the most vulnerable (individuals at highest risk for a poor outcome), 4. herd immunity, or 5. some combination of the above.
Because of vectors in other animals, it’s impossible to eradicate these viruses (unless you start vaccinating mosquitoes and bats, I guess). I think it also doesn’t make sense to talk about eradicating the vectors, either. Mosquitos are a nuisance, in addition to carrying harmful diseases, but I’m sure they serve some sort of useful purpose. I can’t imagine making a life form extinct because they’re a nuisance to humans.
So, let’s talk about vaccination/protection of high risk groups and herd immunity. Obviously, we’re far enough into this pandemic that public health officials and governments have already made these decisions and have decided a course of action. I’m not second guessing the approach or even throwing stones with perfect hindsight.
Higher risk individuals include older adults 65 years and older and those with serious underlying medical conditions; things like heart conditions, diabetes, obesity, immunocompromised, etc. To those we would add pregnant women for Zika because it can be transferred intrautero.
Herd immunity is when a specific population reaches a percentage of individuals who are protected from the disease either by vaccine or through natural immunity. At that point, for those who are not immune, the risk of disease is low, because there are so few carriers. Thus, those at high risk are protected by those who have been previously exposed. Debate remains on what a realistic percent of the population (vaccinated + recovered with antibodies) would be needed to constitute herd immunity for coronavirus.
The War in Panama
With IBM’s Zika initiative in Panama, we were able to develop a real-time phone-based application with geolocation marking, which could reduce both the severity and duration of outbreaks when fully implemented. By replacing the labor-intensive and error-prone recording and reporting, the data reached the decision-makers in hours instead of weeks. Public health officials at the national level were able to compare real-time location reports of disease-carrying mosquitoes with the real-time reporting of hospitalized clinical cases. In the war on the Zika virus, these officials then directed resources to those specific locations to eradicate mosquitoes in that area.
So, instead of a broad brush approach to fighting a disease, they concentrated their efforts on problem areas and potential problem areas. In doing so, they were better able to focus resources and were able to more quickly snuff out the hot spots.
With all of that as background, I’m going to try to draw some parallels between the Zika pandemic and our current COVID pandemic. One study in the Journal of Midwifery & Women’s Health conducted a survey of the clinical literature and determined, “There are significant parallels between [the Zika virus] disease and COVID‐19 in terms of limited diagnostic techniques, therapeutics, and prognostic uncertainties.” In both pandemics, patients and clinicians lacked information to make informed decisions. Public health messaging was often contradictory within the same institution. Disinformation was disseminated in the social media platforms of each pandemic’s time. Serious scientific debate even led to conspiracy theories. It’s not hard to imagine that each of these negatively impacted responses to the viruses in the vulnerable or high-risk individuals.
A Comparison of Zika Virus and COVID‐19: Clinical Overview and Public Health Messaging
| Zika Virus Disease | COVID‐19 | |
|---|---|---|
| Vector | Flavivirus: vector Aedes aegypti and Aedes albopictus mosquitoes 3 | Coronavirus: droplets, fomites 74 |
| Transmission | Mosquitoes are primary vector
Sexual transmission 10 Transmitted by blood transfusion, laboratory exposure 9 |
Transmitted by respiratory droplets 74
Likely airborne transmission 75 |
| Vertical transmission during pregnancy | Vertical transmission from pregnant person to fetus occurs, and congenital infection is likely 9 | Vertical transmission/congenital infection is unlikely 76 |
| Symptoms | Often asymptomatic; mild flu‐like symptoms such as fever, arthralgia, rash, and conjunctivitis 3 | Asymptomatic; also mimics normal rhinorrhea and physiologic dyspnea of pregnancy 65 |
| Diagnostic testing | RT‐PCR, NAAT, PRNT, IgM serologies 32
High rate of false negatives and positives 26 Cross‐reaction of immunoglobulin serologies with other endemic flaviviruses, such as dengue fever virus 26 Perinatal diagnosis limited by sensitivity and specificity of ultrasound for detection of viral injury 20 |
RT‐PCR, NAAT, IgM serologies 42
Sensitivity varies according to time from exposure, sampling technique, specimen source 76 Rapid antigen tests (COVID‐19 Ag Respi‐Strip) available, but there are concerns about their validity, accuracy, and performance 76 Continued lack of testing capacity and laboratory reagents 42 |
| Therapeutics | Supportive care
Congenital Zika syndrome requires specialized care, physical therapy, pharmaco‐therapeutics for seizure disorders, correction/prosthetics for auditory and optical deficits 23 |
Supportive care
Remdesivir appears safe in pregnancy Other therapies (ribavirin, baricitinib) are teratogenic, embryotoxic 39 |
Abbreviations: COVID‐19, coronavirus disease 2019; IgM, immunoglobulin class M; NAAT, nucleic acid amplification test; PRNT, plaque reduction neutralization test; RT‐PCR, reverse transcription polymerase chain reaction test.
This article is being made freely available through PubMed Central as part of the COVID-19 public health emergency response. It can be used for unrestricted research re-use and analysis in any form or by any means with acknowledgement of the original source, for the duration of the public health emergency. (edited by the author)
In our Zika experience in Panama, the door-to-door inspections looked for mosquitos. Today, we use COVID tests to look for the coronavirus. Both look for evidence of the virus, referred to as vector inspection. The vector inspection looks for evidence of potential carriers of the virus and conditions that allow it to thrive.
Comparing COVID-19 to Previous Pandemics
Compared to other recent epidemics, COVID-19 rates as one of the more pervasive in terms of countries affected and number of cases identified. Fortunately, the Case Fatality Rate (CFR) is lower than other major epidemics.
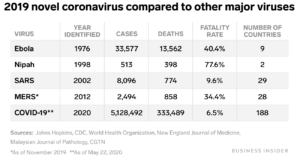
Source: How the Coronavirus Compares to SARS, Swine Flu, and Other Epidemics
Coronavirus ranks more deadly than a couple of other diseases not included in this chart. The 2009 outbreak of swine flu (H1N1) infected between 700 million and 1.4 billion people globally, but had a CFR of 0.02%. Also not in this chart is the 500,000 suspected cases of the Zika virus in 2015 and 2016 and its 18 deaths. To bring COVID-19 more up-to-date, as of December 2021, the Worldometer coronavirus tracking website put the number of cases at 267,921,597 with 5,293,306 deaths for a calculated CFR of 1.98%. Because COVID-19 can be asymptomatic as described in the Journal of Midwifery & Women’s Health study, they may not even know they are sick. There is no reason for these people to seek out a test so they don’t end up a part of the denominator. In other words, this scenario can lead to case rates for COVID-19 being higher than the statistics show.
In the early phases of a pandemic, data from epidemiology modeling, clinical diagnosis and treatment efficacy are often scarce. Strategies in the initial phase include ramping up testing and reporting, communication, and trying to prepare the anticipated capacity for vaccine, testing and treatment. Everyone then, whether conscious or not, makes an individual risk assessment based on their understanding of risk severity, their perceived ability to deal with the threat and the consequences of the threat. In today’s society, these beliefs are then strengthened or weakened by the diet of social media and information sources.
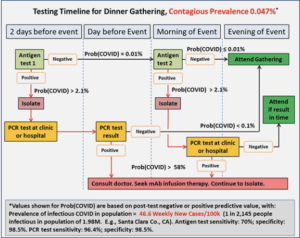
COVID tests evaluate the presence of the coronavirus. Depending on the type of test administered, a positive result will either indicate that the patient has an active infection (rapid molecular PCR test or lab antigen tests) or has had an infection at some point (antibody test).
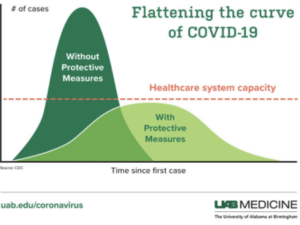
If a person has symptoms consistent with COVID and a positive viral antigen test, action is warranted. That action will be to kill the virus and stop the spread. But, because coronavirus is so contagious, individuals with mild symptoms and no other underlying conditions, experts recommend the assumption of a positive test and quarantine themselves for 10 days to two weeks. [UPDATE: In late December 2021, the CDC shortened the recommended isolation period for individuals who have COVID to 5 days followed by 5 days of masking around others. For those who are exposed to known cases of the virus, the CDC recommends a 5 day quarantine plus 5 days of masking for the unvaccinated. Or, 10 days of masking if vaccinated and boosted.] Still other experts recommend treating asymptomatic individuals if they have a positive COVID antigen test. (Research, however, shows that the infectivity of asymptomatic individuals is weak. The challenge, however, is distinguishing asymptomatic from presymptomatic which is contagious.) The virus is killed by treating the patient, allowing the body’s defense system to mount a response, and isolate the patient while they are contagious. Prevention and early intervention are the keys to managing the pandemic. This is the now familiar, “flattening of the curve.”
 In dealing with Zika, public health recommendations include taking precautions at home that would prevent the incubation and growth of mosquitoes – eliminate standing water in your yard, remove potential reservoirs like old tires. Similarly, recommendations to reduce the spread of the coronavirus include physical distancing, masks and increased hygiene, like hand-washing and safe disposal of used tissues.
In dealing with Zika, public health recommendations include taking precautions at home that would prevent the incubation and growth of mosquitoes – eliminate standing water in your yard, remove potential reservoirs like old tires. Similarly, recommendations to reduce the spread of the coronavirus include physical distancing, masks and increased hygiene, like hand-washing and safe disposal of used tissues.
https://www.news-medical.net/health/How-does-the-COVID-19-Pandemic-Compare-to-Other-Pandemics.aspx
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8242848/ (“External factors such as social networks and informational sources can either amplify or undermine risk perception.”)
https://www.city-journal.org/how-rapid-result-antigen-tests-can-help-beat-covid-19
What I don’t see in the current COVID pandemic is a focused, data-driven, targeted approach. Even in Panama, the public health approach to the Zika pandemic was not a one-size-fits-all. It was impractical – because resources are limited – to fight mosquitoes on every front and it was impossible to eliminate all possible vectors. So, resources were dedicated to those at highest risk based on geography and underlying conditions.
COVID-19 Public Health and Social Measures
With the COVID-19 pandemic, it is likewise impractical to keep everyone from ever getting sick. What we’ve learned is that it makes more sense to prioritize public health intervention to the most vulnerable and to populations at risk to the poorest medical outcomes. If we follow the economics, we have the data to justify dedicating more resources and control measures to: 
- Areas of high population density– geographic as well as situational – cities, public transportation and air travel.
- Institutions which have people with underlying conditions which would contribute to adverse outcomes if they contracted coronavirus – hospitals, clinics
- Individuals with a higher risk of mortality if they contract COVID-19, namely the elderly in nursing homes, retirement communities.
- States with climates more conducive to coronavirus replication. The WHO warns that the virus spreads in all climates, but there are seasonal variations which show spikes in winter months
- Individuals with symptoms have a higher risk of transmitting the disease to others. Testing should be focused on this population and action taken quickly to isolate and treat.
It appears that the WHO June 2021 interim recommendations are leaning in this direction. New recommendations include public health and social measures “tailored to local contexts”. WHO guidance dictates that “[Public health and social] measures should be implemented by the lowest administrative level for which situational assessment is possible and tailored to local settings and conditions.” In other words, evaluating data at the most granular level available and taking action. This publication also further narrows down the focus in a “new section on considerations for individualized public health measures based on a person’s SARS-CoV-2 immunity status following COVID-19 vaccination or past infection “.
Could COVID Follow Zika’s Trend?
Case Counts of Zika in US and Territories
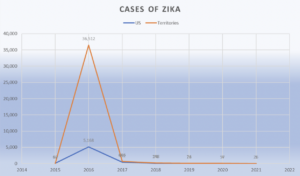
Panama and worldwide data show similar trends for Zika cases. The typical progression is that pandemics lessen to epidemics, then endemics with periodic outbreaks. Today, we are able to look back at the Zika pandemic. I offer a word of hope. With data, experience and time, the coronavirus, like the Zika virus and all viruses before that, will run its course.
Additional Reading: Interesting, but Just Didn’t Fit
How 5 of the World’s Worst Pandemic Ended from the History Channel
Brief History of Pandemics (Pandemics Throughout History)
How do pandemics end? History suggests diseases fade but are almost never truly gone
Finally, Another Weapon Against Covid
How Poop Offers Hints About the Spread of Coronavirus
The Truth Behind the Coronavirus Poop Panic